 Hội Nội Tiết – Đái Tháo Đường Miền Trung Việt Nam Hội Nội Tiết – Đái Tháo Đường Miền Trung Việt Nam
Hội Nội Tiết – Đái Tháo Đường Miền Trung Việt Nam Hội Nội Tiết – Đái Tháo Đường Miền Trung Việt Nam
HYPOGLYCEMIC DETECTION WITH CONTINOUS GLUCOSE MONITORING IS MUCH MORE EFFECTIVELY THAN FREQUENT CAPILLARY BLOOD GLUCOMETER IN DIABETIC PATIENTS
Nguyen Khoa Dieu Van, Nguyen Dinh Duc, Trinh Ngoc Anh
ABSTRACT
Hypoglycemic detection with continuous glucose monitoring is much more effectively than frequent capillary blood glucometer in diabetic patients
Hypoglycemia is a dangerous and common complication of diabetes, many events of which could be undetected with frequent blood glucose tests. A continuous glucose monitoring (CGM) device can detect nocturnal and asymptomatic hypoglycemic episodes more effectively. Objective: to compare the effectiveness of continuous glucose monitoring (CGM) and self-monitored capillary blood glucose (CBG) on detection of hypoglycemic episodes. Research design and methods: we studied on diabetic patients treated with insulin or oral agents, who were monitored in 6 consecutive days using both CGM and CBG. Results:43 patients were 46 ± 17 years old with an HbA1c of 8.15 ± 1.98%. Each patient was monitored for an average of 144 hours. In this group, 32/43 (74.4%) of these had hypoglycemic episodes with an average of 0.77 ± 0.53 episodes/day, of those events, 21.3% were severe and 31.5% were at night.SMBG revealed that 44.2% of the patients had experienced hypoglycemia Meanwhile CGM found hypoglycemia in 74.4% of patients. CGM detected significantly higher percentages of hypoglycemic episodes than capillary blood glucose measurements with 144 events vs 40 events, in which severe episodes were 31 and 6, respectively. 41.8% of patients experienced asymptomatic hypoglycemic episodes and 27.9% experienced nocturnal hypoglycemic events recorded by CGM but had no data in capillary blood glucose diary. Also in these patients, the mean duration of hypoglycemia was 1.22 ± 0.28 hour/day with longest time 6.79 ± 1.22 hour/day per patient. Conclusions:In diabetic patients, CGM showed a higher number of hypoglycemicevents than did CBG, especially asymptomatic and nocturnal events. CGM is very useful in detecting hypoglycemic events effectively and providing valuable information for clinical doctors.
Keywords:continuous glucose monitoring, hypoglycemic.
Main correspondence:Van Nguyen Dieu Khoa
Submission date: 9 Feb 2017
Revised date: 21 Feb 2017
Acceptance date: 15Mar 2017
I. Background
Hypoglycemia is a dangerous and common complication of diabetes. According to ADA reports, 2-4% of diabetic death related to hypoglycemia, many events of which cannot be detected. Hypoglycemia can be very dangerous, if not early detected and treated, especially in elderlies, patients with cardiovascular, liver or renal diseases [1,2]. Asymptomatic hypoglycemia is commonly seen in diabetic patients with multiple hypoglycemia episodes in the past and tend to be more severe. However, they are very difficult to be detected, especially at night [3].
There are some available methods to diagnose hypoglycemia: self-monitoring of blood glucose using capillary blood glucometer (CBG) and continuous glucose monitoring (CGM). The latter is considered more effective in detecting asymptomatic and nocturnal hypoglycemia events. Recent guidelines from ADA and AACE recommend the use of CGM in patients with frequent and asymptomatic hypoglycemic episodes [3,4,5]. In this study, we would like to compare the effectiveness of hypoglycemia detection using CGM and frequent CBG.
II. Material and methods
1.Patients
The study conducted by the department of diabetes and endocrinology at Bach Mai hospital, Hanoi, Vietnam, enrolled 43 diabetic patients with past medical history of hypoglycemia. Patient demographics included age, past medical history, diabetic duration, body weight, height, blood pressure and baseline tests such as fasting blood glucose, HbA1c, lipid profile, renal and liver function tests. The exclusion criteria included pregnant women, patients with acute disease (infection, acute myocardial infarction, acute hyperosmolar hyperglycemic state or ketoacidosis) or patients using glucocorticoid or hyperglycemia induced medications.
2. Glucose monitoring
Each patients participated individual training by our trained research physicians and technician. All patients were taught to self-monitor their blood glucose at least 4 times/day with Accuchek Active or Freestyle glucometer. The 4 measurements were conducted 30 minutes before meals and bedtime or whenever the patient had symptoms of hypoglycemia. The participants were also trained about how to conduct CGM using Medtronic iPro2 device. This system is composed of a disposable subcutaneous glucose-sensing device and an electrode impregnated with glucose oxidase connected with a lightweight monitor. Interstitial glucose levels in subcutaneous tissue, within a range of 2.2 to 22.2 mmol/L, were measured electrochemically every 10 seconds and an average value stored every 5 minutes, providing up to 288 measurements per day. The CGM system does not display glucose values; data were stored in the monitor and downloaded and printed after removing the sensor. A minimum of 4 daily blood glucose calibration values were introduced to the CGM sensor. Patients were trained in recording of time, of food intake, exercise periods, insulin injections, and symptomatic hypoglycemic events [6]. Patients were provided with user manuals and advised to contact our research physicians and technician at any time of the day if a problem arose.
3. Study design
After 6 days, the sensor were removed and data were collected and analyzed using Medtronic specific software [6]. The CBG results also were recorded using patients’ diary and glucometer history. With any hypoglycemic events (blood glucose ≤ 3.9 mmol/l on either CBG or CGM), our physician retrospectively asked patients on whether or not the hypoglycemic events occurred with warning symptoms, preceded treatment, meals or exercises related.
We also classified the hypoglycemic events into groups by daytime (from 6 am to 11 pm) or nighttime (from 11 pm to 6 am), symptomatic or asymptomatic and severity. The severity of hypoglycemic events were classified based on the lowest blood glucose levels: mild hypoglycemia (BG from 2.8 to 3.9 mmol/l) and severe one (BG <2.8 mmol/l).
4. Statistical analysis
SPSS version 20.0 was used for data analysis. The data on continuous variables with normal distribution are presented as mean±SD. Categorical data are shown as counts and percentages. Continuous variables were analyzed by means of ANOVA if they were normally distributed and by means of nonparametric tests if their distribution was not normal. Frequency variables were compared using the χ2 test. Values of p < 0.05 were considered statistically significant.
III. Results
1.Demographics and baseline characteristics:
In total, 43 patients completed the study, with 27 female patients (62.8%), patients’ average age was 46 ± 17 (years old). There were 18 type 1 diabetic patients (41.9%) and 25 type 2 diabetic patients (58.1%).
The mean diabetic duration was 8.53 ± 7.0 (years), in which the mean duration of type 1 diabetes was 6.0 ± 6.37 (years) and 10.2 ± 7.02 (years) for type 2 diabetes. Nearly half of those patients (20/43, 46.5%) used insulin only, 19/43 patients (44.1%) used both insulin and oral agents. The mean HbA1c of the group was 8.15 ± 1.98%.
2. Characteristics of hypoglycemic events recorded by CGM
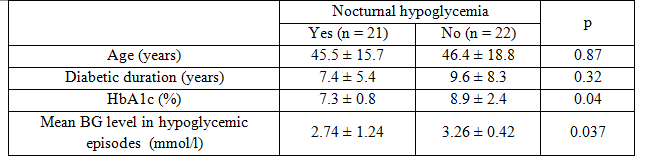
We found 32/43 (74.4%) of our patients had hypoglycemic events with 146 hypoglycemic episodes detected by CGM; on average, each patients had 0.77 ± 0.53 events per day. On severity, 78.7% (115/146) episodes were mild and 21.3% (31/146) were severe ones. Concerning time, 31.5% (46/146) events occurred at night and 68.5% (100/146) events in daytime. Patients with nocturnal hypoglycemia had significantly lower HbA1c level compare to those without nocturnal hypoglycemia (7.3 ± 0.8% vs 8.9 ± 2.4%, p = 0.04) and the mean blood glucose level in nocturnal events was significantly lower than daytime events (2.74 ± 1.24 mmol/l vs 3.26 ± 0.42 mmol/l,
p = 0.037).
Table 1: Comparison between groups of patients with or without nocturnal hypoglycemia
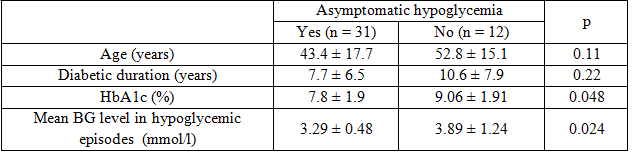
 In 146 events, we also found that 75.5% (110/146) events occurred silently without any symptoms, only 24.5% (36/146) events preceded by warning symptoms of hypoglycemia. The mean blood glucose level in unrecognized events was significantly lower than this level in symptomatic events (3.29 ± 0.48 vs 3.89 ± 1.24 mmol/l, p = 0.024). Compare to group of patients who have symptomatic hypoglycemia, patients with unrecognized hypoglycemia had significantly lower HbA1c levels and no significantly different in age and diabetic duration. In 110 episodes of unrecognized hypoglycemia, 88/110 (80%) were mild, 22/110 (20%) of those were severe, 72/110 (65.5%) occurred at daytime and 38/110 (34.5%) occurred at night.
In 146 events, we also found that 75.5% (110/146) events occurred silently without any symptoms, only 24.5% (36/146) events preceded by warning symptoms of hypoglycemia. The mean blood glucose level in unrecognized events was significantly lower than this level in symptomatic events (3.29 ± 0.48 vs 3.89 ± 1.24 mmol/l, p = 0.024). Compare to group of patients who have symptomatic hypoglycemia, patients with unrecognized hypoglycemia had significantly lower HbA1c levels and no significantly different in age and diabetic duration. In 110 episodes of unrecognized hypoglycemia, 88/110 (80%) were mild, 22/110 (20%) of those were severe, 72/110 (65.5%) occurred at daytime and 38/110 (34.5%) occurred at night.
Table 2: Comparison between groups of patients with or without unrecognized hypoglycemia
 Also in these patients, the mean duration of hypoglycemia was 1.22 ± 0.28 hour/day with longest time was 6.79 ± 1.22 hour/day per patient.
Also in these patients, the mean duration of hypoglycemia was 1.22 ± 0.28 hour/day with longest time was 6.79 ± 1.22 hour/day per patient.
3. Hypoglycemic detection with CGM versus CBG
SMBG revealed that 44.2% (19/43) of the patients had experienced hypoglycemia meanwhile CGM found hypoglycemia in 74.4% (32/43) of patients. All patients with hypoglycemia detected by CBG were also recorded by CGM.
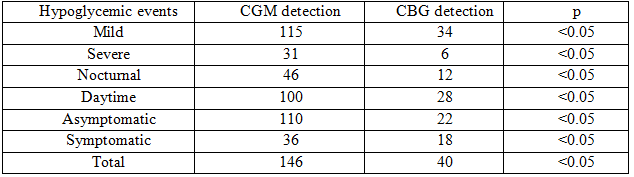
CGM detected significantly higher percentages of hypoglycemic episodes than capillary blood glucose measurements with 144 events vs 40 events, in which severe episodes were 31 and 6, nocturnal events were 40 and 12, and unrecognized events were 110 and 22, respectively. In our study, 27.9% experienced nocturnal hypoglycemic events and 41.8% of patients experienced asymptomatic hypoglycemic episodes recorded by CGM but had no data in capillary blood glucose diary.
Table 3: Hypoglycemia detection with CGM vs CBG
 Iv. Discussion
Iv. Discussion
Hypoglycemia has many deleterious effects in the development of acute cardiovascular complications in diabetes. These events should be soon recognized and managed for the safety of diabetic patients. In our study, hypoglycemia episodes were seen in 74.4% patients (88% type 2 and 64% type 1 diabetes), with average of 0.77 ± 0.53 events/day. Naik et al saw a similar results at 80% type 1 patients using iPro2, while Tsirona et al studied on 17 type 2 diabetic patients and recorded 58.8% of them had hypoglycemia [7,8]. On severity, 31/146 (21.3%) events were severe episodes. This prevalence was lower than JDRF’s study in which 30.5% events in were severe ones [9]. The difference in study samples (ours were both type 1 and 2 but JDRF focus on type 1 diabetes only) and sample size (46 vs 165) might lead to our lower prevalence of severe hypoglycemic events [9].
In diabetic patients, the attenuated sympatho-adrenal response to hypoglycemia might cause the clinical syndrome of hypoglycemia unawareness. These patients might not have warning signs or symptoms and therefore do not recognize the episodes. Affected patients are at six fold increased risk of severe iatrogenic hypoglycemia during treatment [3]. The proposed benefits of CGM over CBG were demonstrated in many studies. CGM, with advantage of continuous measurements, might facilitate the detection of all unrecognized hypoglycemic episodes despite some questions on its accuracy [3]. Our study was designed to examine the real superiority of CGM in detecting hypoglycemic events in diabetic patients compare to CBG. We used both standard method with capillary blood glucometer and the newer method with retrospective CGM using iPro2 in the same group of patients. We took data in 6 consecutive days and asked our patients on every hypoglycemic events.
Our findings showed clearly that asymptomatic hypoglycemia were very common in diabetic patients, with the three quarter of events (75.5%) occurred without warning symptoms. Our findings were agreed with many previously published studies demonstrated the utility of CGM in hypoglycemia detection. Schiaffini et al used CGMS in 18 children with type 1 diabetes, he found that using CGM system could detect a significantly higher number of asymptomatic hypoglycemic events in comparison with standard glucometer (3.6 ± 2.3 vs 0.7 ± 0.9; p<0.0001) [10]. Chico et al studied in 70 diabetic subjects found that CGM could detect unrecognized hypoglycemia in 62.5% of type 1 diabetic and in 46.6% of type 2 diabetic patients [11].
Nocturnal hypoglycemia is also a common problem for diabetic patients. According to many studies (DCCT 1991; Bolli et al 1993; David et al 1997; Matyka et al 1999), it is estimated that up to 75% of hypoglycemic episodes associated with coma or seizures occur at night when the counter regulatory response is impaired [5].
It is believed that the real prevalence of nocturnal hypoglycemia might be very high and would be underestimated with SMBG due to its intermittence and dependence on the initiative of the patient [9]. The introduction of CGM provide useful method to measure blood glucose every 5 minutes and lead to higher level of monitoring. Many studies showed the prevalence of nocturnal hypoglycemia detected with CGM was up to 68% (Boland et al 2001; Yates et al 2006; Guillod et al 2007; Amed et al. 2011) [5]. In Chico’s study, he found that 73.7% of all hypoglycemic events occurred at night. The prevalence of nocturnal hypoglycemia using CGM in our study was lower at 31.5% with 85.7% of those were asymptomatic events [11]. Meanwhile, if using CBG we could just detect 12 nocturnal events, which was much lower than that of CGM detection.
Another superiority of CGM over CBG is that the CGM system could estimate the duration of each hypoglycemic events. Capillary blood glucometer just provides blood glucose at the time the test was done and it could not tell how long the hypoglycemic episode did happen. The use of CGM could extract the information and provide the duration of each hypoglycemic events from its beginning to end [9]. As in our study, the mean duration of hypoglycemia was 1.22 ± 0.28 hour/day with longest time was 6.79 ± 1.22 hour/day per patient. This information were clinically useful for our physicians.
Several limitations existed in our study. In our country, the use of CGM just started for 2 years and its accuracy in our practice was remained the subject of debate. Although frequent calibration with glucometer, but when compared with actual blood glucose values, CGM devices have an inaccuracy of approximately 15%, this number is worse during hypoglycemia [9]. Regarding to study design, we conducted our study on a relatively small number of patients including both type 1 & 2 diabetes, it was inadequate to get significant differences between groups. Other errors might be caused by deficits in training, our patients retrospectively recalled their symptoms, their diaries recorded…. Thus, a large-scale prospective clinical trial is required to further test the efficacy and utility of CGM over CBG.
V. Conclusion
In diabetic patients, CGM showed higher number of hypoglycemicevents than did SMBG, especially asymptomatic and nocturnal events. CGM is very useful in detecting hypoglycemic events effectively and providing valuable information for clinical doctors.
REFERENCES
- Zammitt NN, Frier BM: Hypoglycemia in Type 2 diabetes: pathophysiology, frequency, and effects of different treatment modalities. Diabetes Care 2005; 28:2948-61.
- Howard AW: Use of continuous glucose monitoring in the detection and prevention of hypoglycemia. Journal of Diabetes Science and Technology, Volume 1, Issue 1, Jan 2007.
- Pratik C, Sharmin R, et al: Real-time continuous glucose monitoring significantly reduces severe hypoglycemia in hypoglycemia-unaware patients with type 1 diabetes. Diabetes Care 36:4160-4162, 2013.
- William HP, Anne LP, et al: The impact of real-time continuous glucose monitoring in patients 65 years and older. Journal of Diabetes Science and Technology 2016, Vol. 10(4) 892 –897.
- Nalinee P, Naeti S, et al: Systemic review and meta-analysis of the effectiveness of continuous glucose monitoring (CGM) on glucose control in diabetes. Diabetology & Metabolic Syndrome 2013, 5:39.
- Garry Scheiner MS: CGM retrospective data analysis. Diabetes Technology and Therapeutics, Volume 18, Supplement 2, 2016.
- Juvenile Diabetes Research Foundation Continuous Glucose Monitoring Study Group: Prolonged nocturnal hypoglycemia is common during 12 months of continuous glucose monitoring in children and adults with type 1 diabetes. Diabetes Care 33:1004-1008, 2010.
- Tsirona S, Pappas C, et al: Detection of hypoglycemia in type 2 diabetic patients. Endocrine Abstracts (2016) 41 EP527.
- Juvenile Diabetes Research Foundation Continuous Glucose Monitoring Study Group: Effectiveness of continuous glucose monitoring in a clinical care environment. Diabetes Care 33:17-22, 2010.
- Schiaffini R, Ciampallini P, et al: The continuous glucose monitoring system (CGMS) in type 1 diabetic children is the way to reduce hypoglycemic risk. Diabetes Metab Res Rev. 2002 Jul-Aug;18(4):324-9.
- Chico A, Vidal-Rios P, et al: The continuous glucose monitoring system is useful for detecting unrecognized hypoglycemia in patients with type 1 and type 2 diabetes but is not better than frequent capillary glucose measurements for improving metabolic control. Diabetes Care 2003 Apr;26(4):1153-7.