Hội Nội Tiết – Đái Tháo Đường Miền Trung Việt Nam Hội Nội Tiết – Đái Tháo Đường Miền Trung Việt Nam
Hội Nội Tiết – Đái Tháo Đường Miền Trung Việt Nam Hội Nội Tiết – Đái Tháo Đường Miền Trung Việt Nam
EVALUATION OF DIABETIC FOOT BY WOUNDS, ISCHEMIA, AND FOOT INFECTIONS (WIfI) CLASSIFICATION SYSTEM
Huynh Le Thai Bao 1,2, Nguyen Hai Thuy 1
1 Hue University of Medicine and Pharmacy
2 Duy Tan University
DOI: 10.47122/vjde.2022.53.8
ABSTRACT
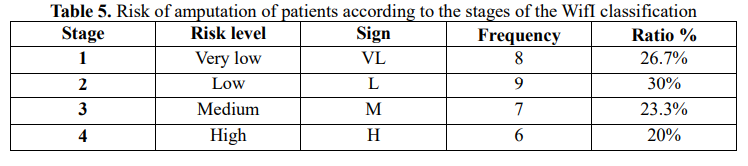
Objective: To describe the characteristics of wounds, ischemia, and foot infections classification system (WIfI) in patients with diabetic foot and analyze risk factors relating to the WIfI classification in these patients. Methodology: A cross-sectional descriptive study, 30 patients with diabetic foot disease at Hue Central Hospital from December 19, 2021 to April 29, 2022. Results: Prevalence of amputation risk WIfI classification is 26.7 in stage 1 (VL), 30% in stage 2 (L), 23.3% in stage 3 (M) and 20% in stage 4 (H). The related factors of the WIfI classification stages were HbA1C (p=0.035), ABI (p=0.05), TBI (p=0.01), TP (p=0.01). The regression model is described by the equation: Risk of amputation = 3.701 – 0.788ABI – 1.260TP. Conclusion: It is necessary to apply the WIfI classification for the assessment of patients with diabetic foot in Vietnam, paying special attention to the TP and ABI index.
Keywords: WIfI, classification, diabetic foot
Main correspondence: Huynh Le Thai Bao
Submission date: 19th Oct 2022
Revised date: 19th Nov 2022
Acceptance date: 19th Dec 2022
Email: [email protected]
Tel: 0888838539
1. BACKGROUND
Diabetes mellitus (DM) is a chronic disease, causing many dangerous complications and a huge burden on the health, finances of the patient, family and society. In particular, diabetic foot is a dangerous complication, increasing the length of hospital stay and the cost of medication for the patient. About 5-10% of diabetic foot patients have foot ulcers. Diabetic foot pathology is very diverse, the pathogenesis has three main factors: Peripheral vascular disease (including micro and macro vessels), peripheral neuropathy, and infectious complications [1].
These three factors combine to make ulcers difficult to heal and increase the rate of amputation.
Diabetic foot disease is one of the leading causes of non-traumatic amputation. Epidemiological statistics show that 85% of amputations begin with an ulcerative lesion [6].
The rate of amputation in diabetic foot patients according to worldwide studies is quite high. According to research by Wukich (2013), this rate is 51% [5], according to Richard (2011) 35% [4], according to Le Tuyet Hoa (2005) 52.9% [5] and Huynh Tan Dat (2018) is 46.5% [6].
The three most common factors associated with amputation are: ulcer depth, infection, and lower extremity ischemia.
Based on these factors, in the world there are many different classifications of diabetic foot, in order to plan treatment, predict the outcome of ulcer healing and assess the risk of amputation.
The commonly used grades/scales are: Rutherford, Fontaine, Wegner, University of Texas. Two clinical grading systems that include factors such as pain at rest, ischemic ulceration, and necrosis are Rutherford and Fontaine. Although these scores can help identify patients at risk for amputation and death, they are not detailed enough to stratify risk. The Wegner scale assesses ulcer depth and the presence of infection but does not assess the degree of ischemia.
The University of Texas Scale can assess ulcer severity, infection, and lower extremity ischemia, and is a qualitative rather than quantitative grading scale. Since 2014, the European Society of Vascular Surgeons (SVS) has proposed a new classification of WIfI (Wound, Ischemia, and foot Infection) [4].
This classification is based on degree of ischemia, extent of wound, gangrene and infection; used to assess the risk of amputation within 6 months or 1 year [4].
The systematic study by van Reijen (2019) showed that the amputation rates according to the four stages of WIfI grades from 1 to 4 were 0%, 8%, 11%, 38%, respectively [4].
In addition, the WIfI grading also helps to predict ulcer healing in diabetic foot disease, Weaver’s study (2019) shows that the ulcer healing rate of stage 1/2 WIfI is much higher than stage 3/WIfI stage 3/ 4, 77.3% versus 57.2% [7]. To initially assess the distribution of diabetic foot disease as well as factors related to this WIfI category, we conducted a study with the following objectives: 1,
Describe the characteristics of the WIfI classification in patients with diabetic foot. And 2 Analysis of some factors related to the WIfI classification in patients with diabetic foot disease.
2. RESEARCH SUBJECTS AND METHODS
2.1. Subject: Sample subjects: Diabetic patients with foot disease at Hue Central Hospital from December 19, 2021 to April 29, 2022
Sample size: 30 patients
2.2. Research Methods: Descriptive cross-sectional study and convenience sampling
2.3. Data analysis:
Statistics using SPSS 20.0 software and Microsoft Excel 2003. Analyze univariate relationships by Person’s Chi-Square (χ2) test with significance p < 0.05. Multivariable logistic regression analysis for related factors.
2.4. Key variables:
WIfI classification, ABI, TBI, TP, white blood cell count (WBC) were applied according to the European Society of Vascular Surgery SVS 2014. [4]
The goal of controlling blood glucose and blood lipids by HbA1c and plasma glucose indexes is applied according to the American Diabetes Association’s (ADA) Standards of Medical Care in Diabetes in 2022.
3. RESULTS AND DISCUSSION
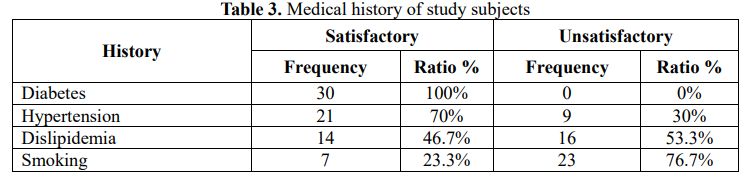
3.1. General information of research subjects


3.2. Wound, ischemia and foot infection (WIfI) characteristics of study subjects
3.3. Relationship between stages of the WIfI classification and risk factors

4. DISCUSSION
4.1. Characteristics of the WIfI classification in patients with diabetic foot
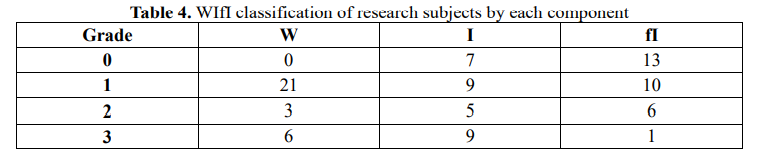
According to each component W, I and fI, most patients have ulcers (W) of all degrees, however, in terms of severity of the disease, component I (ischemia) accounts for the severity at grade 2 and grade 3 higher. Therefore, clinically, it is necessary to investigate the degree of foot ischemia with tools such as TP, ABI, TBI because sometimes the ischemia appears in the foot before the ulcer.
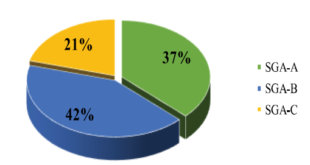
Compare the components with the WIfI classification of the risk of amputation [4] of the patients in the study. Disease stages 1,2,3,4, corresponding to very low, low, high and very high risk levels (VL, L, M, H), there are 43.3% of hospitalized patients at amputation risk of moderate and high stage (3 and 4), this figure in the study of Weaver et al. is 70.67% [7], of Caitlin W. Hicks et al. 47.6% [8], William P Robinson et al. is 53% [10], Luke X. Zhan is 55.7%. Thereby, it shows that diabetics with foot disease are most at risk of amputation, these are the subjects that need to be continued to be monitored and carried out prospectively in the near future.
4.2. Relationship between the stage of the WIfI classification and risk factors
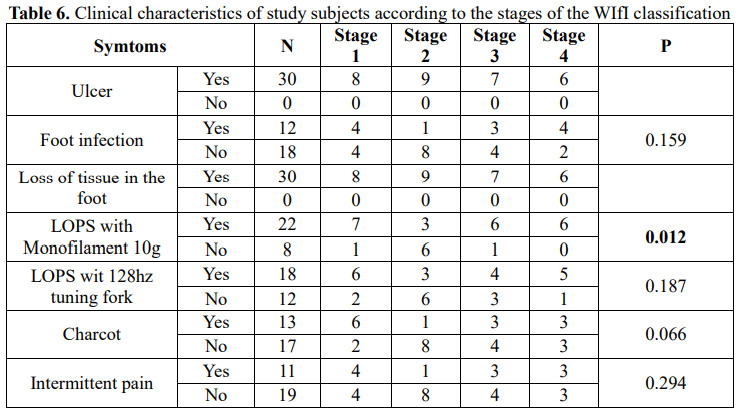
The 10g Monofilament Foot Sensory Examination method detected statistically significant associated loss of protective sensation (LOPS) across different stages of diabetic foot (p=0.012). In the study of Caitlin W. Hicks, LOPS (93.2%) was statistically significant with p<0.01 [8].
In the study of William P. Robinsot [10], this is not statistically significant (p=0.92). LOPS requires special attention in screening for diabetic foot because in many patients there is no trace but signs of loss of protection and
manifestations such as ischemia. LOPS has not been observed in many studies that are statistically significant in association with disease stages of diabetic foot, so many classifications do not include this criterion.
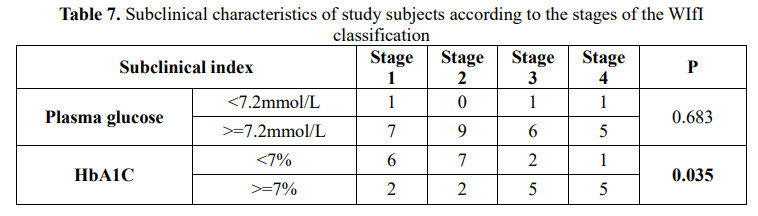
HbA1c was related with risk levels according to amputation stage in patients with diabetic foot (p=0.035). M. Libby Weaver and William P. Robinson have the same results in this study (p<0.05) [7],[10].
This is consistent with the pathophysiology of diabetic foot disease where higher HbA1c represents poorer glycemic control leading to worsening of diabetic foot disease through hypoperfusion mechanisms, loss of protective sensation and wound necrosis.
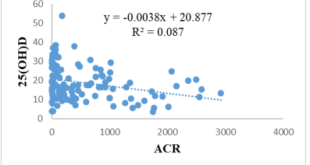
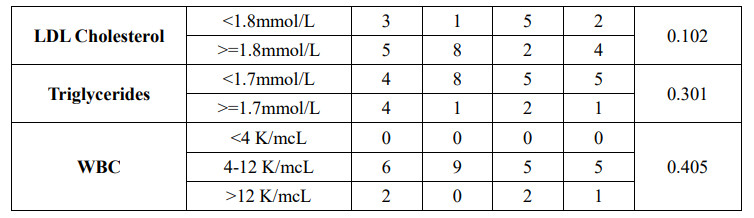
ABI, TBI, TP are all statistically significant in terms of study subjects in the risk stages of limb amputation of the WIfI classification (p is 0.05, 0.01, 0.01, respectively). William P. Robinsot has the same study results when ischemia based on ABI and TP is statistically significant across the stages of WIfI (p<0.01) [10]. This is also consistent with the pathophysiological mechanism when the perfusion is reduced, the earlier and more severe the ulceration and necrosis of the foot occurs. However, the problem and need to be explained is which of the variables ABI, TBI
and TP is more valuable and should be paid more attention.
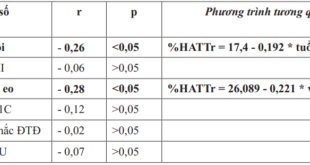
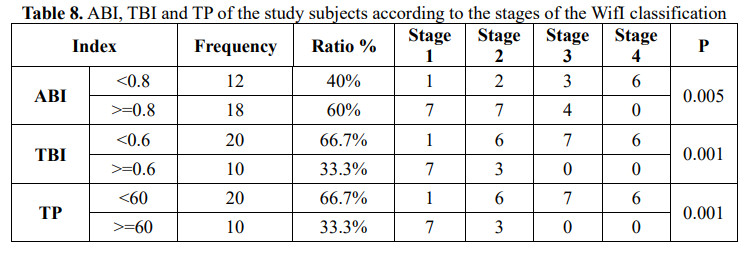
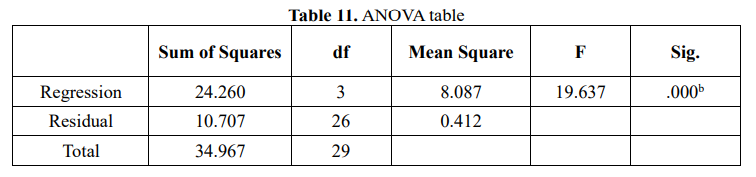
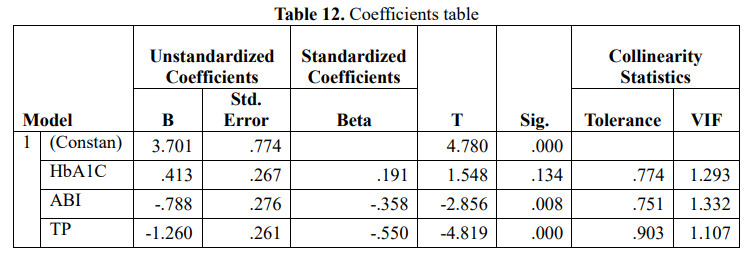
To clarify the factors related to the risk of amputation (according to the WIfI classification), we analyzed the relationship of some factors with the risk of amputation of the patient according to Table 9. Based on the analysis analyzed by correlation coefficient table, variable HbA1C is positively correlated with risk of amputation (. sig<0.05), variables ABI, TBI and TP are inversely correlated with risk of amputation (.sig) <0.001). Based on these related factors, we proceed to build a regression model with the dependent variable being the risk of amputation and the independent variable being the variables HbA1C, ABI, TBI, TP, the results are obtained in Table 10. Thereby, the variables in the model explain 83.3% of the variation in the risk of amputation.
During the analysis, the variable TBI was excluded from the model because of the perfect multivariable addition, and the variable HbA1C was not statistically significant (.Sig>0.05), only two variables ABI and TP were statistically significant, there is also no polylinearity, so the regression equation of the risk of amputation according to the WIfI scale has the form: Risk of amputation = 3.701 – 0.788ABI-1.260TP
Thus, from the equation we can clearly determine, the risk of amputation will increase when the indicators of ischemia in the limb decrease, this result is consistent with the statement in the study of William P. Robinsot et al. the [10]. We do not currently have studies to the contrary on this issue of ischemia.
5. CONCLUSION
5.1. Characteristics of the WIfI classification in patients with diabetic foot
The WIfI classification of amputation risk is 26.7% in stage 1 (VL), 30% in stage 2 (L), 23.3% in stage 3 (M) and 20% in stage 4 (H).
5.2. Relationship between the stage of the WIfI classification and risk factors
The HbA1C concentration has a positive correlation with the risk of amputation, and the ABI, TBI, and TP indexes are negatively correlated with this variable.
Regression equation for amputation risk according to WIFI grace has the form: Risk of amputation = 3.701 – 0.788ABI-1.260TP
It is necessary to apply the WIfI classification in the screening and assessment of diabetic foot disease in Vietnamese people. Special attention to the ABI and TP indexes in this group of patients.
FUNDING
Research is supported by Vingroup Innovation Foundation (VINIF) in code VINIF. 2021.TS.003.
The authors declare that this study received funding from Vingroup Innovation Foundation (VINIF). The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article, or the decision to submit it for publication.
REFERENCES
1. Nguyen Hai Thuy. (2018). University medical textbook: Internal Medicine Pathology. Hue University Press.
2. Warren Clayton, T. A. E. (2009). A Review of the Pathophysiology, Classification, and Treatment of Foot Ulcers in Diabetic Patients. Clinical Diabetes, 2009 Apr 27 (2), 52-58.
3. Wukich DK, H. K., Raspovic KM, Rosario BL,. (two thousand and thirteen). SIRS is valid in discriminating between severe and moderate diabetic foot infections. Diabetes Care, 2013 Nov; 36(11), 3706-3711.
4. Mills, J. L., Sr., Conte, M. S., Armstrong, D. G., Pomposelli, F. B., Schanzer, A., Sidawy, A. N.,. (2014). The Society for Vascular Surgery Lower Extremity Threatened Limb Classification System: risk stratification based on wound, ischemia, and foot infection (WIfI). J Vasc Surg, 59(1), 220-234 e221-222
5. Le Tuyet Hoa. (2005). Risk factors for amputation in diabetic foot ulcers. Practical Medicine, 507-508, 742-750.
6. Huynh Tan Dat. (2018). Prevalence and factors related to lower extremity amputation in diabetic patients with foot ulcers. Thesis of Doctor of Medicine
7. Weaver ML, H. C., Canner JK, Sherman RL, Hines KF, Mathioudakis N, Abularrage CJ,. (2019). The Society for Vascular Surgery Wound, Ischemia, and foot Infection (WIfI) classification system predicts wound healing better than direct angiosome perfusion in diabetic foot wounds. Journal of Vascular Surgery, 68(5), 1473–1481.
8. Caitlin W. Hicks, Joseph K. Canner, Nestoras Mathioudakis, Ronald Sherman, Mahmoud B. Malas, James H. Black, Christopher J. Abularrage, (2018). The Society for Vascular Surgery Wound, Ischemia, and foot Infection (WIfI) classification independently predicts wound healing in diabetic foot ulcers. Journal of Vascular Surgery,Volume 68, Issue 4, 1096-1103.
9. Jeremy D. Darling, John C. McCallum, Peter A. Soden, Raul J. Guzman, Mark C. Wyers, Allen D. Hamdan, Hence J. Verhagen, Marc L. Schermerhorn, (2017). Predictive ability of the Society for Vascular Surgery Wound, Ischemia, and foot Infection (WIfI) classification system after first-time lower extremity revascularizations. Journal of Vascular Surgery,Volume 65, Issue 3, 695-704.
10. William P. Robinson, Lorraine Loretz, Colleen Hanesian, Julie Flahive, John Bostrom, Nicholas Lunig, Andres Schanzer, Louis Messina, (2017). Society for Vascular Surgery Wound, Ischemia, foot Infection (WIfI) score correlates with the intensity of multimodal limb treatment and patientcentered outcomes in patients with threatened limbs managed in a limb preservation center. Journal of Vascular Surgery, Volume 66, Issue 2, 2017, 488-498.e2.
11. Luke X. Zhan, Bernardino C. Branco, David G. Armstrong, Joseph L. Mills, (2015) The Society for Vascular Surgery lower extremity threatened limb classification system based on Wound, Ischemia, and foot Infection (WIfI) correlates with risk of major amputation and time to wound healing. Journal of Vascular Surgery,Volume 61, Issue 4, 939-944