 Hội Nội Tiết – Đái Tháo Đường Miền Trung Việt Nam Hội Nội Tiết – Đái Tháo Đường Miền Trung Việt Nam
Hội Nội Tiết – Đái Tháo Đường Miền Trung Việt Nam Hội Nội Tiết – Đái Tháo Đường Miền Trung Việt Nam
PROGNOSTIC SIGNIFICANCE OF SERUM URIC ACID CONCENTRATION IN PATIENTS WITH ACUTE ISCHEMIC STROKE
Nguyen Dinh Toan, Tong Van Hoan, Nguyen Van Bang, Nguyen Thi Y Nhi*
*Hue University of Medicine and Pharmacy
ABSTRACT
Background : Stroke, especially ischemic stroke, is the third common cause of death worldwide after coronary heart disease and cancer, especially in the elderly. It is also one of the most common causes of disability and dementia. Nowadays, although diagnosis and treatment for stroke have improved, it is still very prevalent. Only 26% survivors recover their independence with work and self – care. Many ischemic risk factors have been used for prognosis; notably, serum uric acid has been used in recent years as prognosis factor for outcome. Current evidence shows that uric acid is a potent antioxidant whose serum concentration increases rapidly after acute ischemic stroke (AIS). Nevertheless, the relationship between serum uric acid (SUA) level and AIS outcome remains controversial.Objective:1) To evaluate serum uric acid concentration in acute ischemic stroke patients, 2) To define correlation between serum acid uric concentration and NIHSS, ischemic size, mRankin. Research design and methods:A total of 84 patients aged from 18 years old, admitted in the Cardiovascular Department at Hue Central Hospital, were evaluated in a prospective study from May 2015 to October 2016. Questionnaire, clinical (Glassgow score, NIHSS, mRankin) and biochemical examinations (routine blood test, glucose level, lipid profile, hs-CRP, serum uric acid) were used.Results:Mean SUA concentration at hospital arrival was (344.86 ± 64.84 μmol/l), at day 3 (323.76 ± 57.47 μmol/l), at day 7 (308.57 ± 42.50 μmol/l) and significantly higher than those of control group. There was a significant positive correlation between SUA and NIH stroke scale score as well as mRankin on day 1 and day 3 (p < 0.05 for both).Conclusions:Our findings support the hypothesis that SUA is more a marker of the magnitude of the cerebral infarction, rather than an independent predictor of stroke outcome.
Keywords: serum uric acid; acute ischemic stroke, mRankin, NIHSS, ischemic size
Main correspondence:Nguyen Dinh Toan
Submission date: 8 Feb 2017
Revised date: 20 Feb 2017
Acceptance date: 15Mar 2017
I. INTRODUCTION
Stroke is a growing disease. According to a recent report, about 780,000 Americans experience a new or recurrent stroke each year; thus, one stroke every 40 seconds on average [8]. Stroke, especially ischemic stroke, is the third common cause of death in the world after coronary heart disease and cancer, especially in the elderly. It is also one of the most common causes of disability and dementia [6], [5], [10]. Nowadays, although diagnosis and treatment for stroke have improved, it is still very prevalent. Only 26% survivors recover their independence with work and self – care [6]. Many ischemic risk factors were used for prognosis; Serum uric acid has been used in recent years as prognosis factor for outcome. Uric acid is the ultimate catabolite of purine metabolism in human and higher primates [2]. It exists in the extracellular compartment as sodium urate, and it is cleared from the plasma through the kidney [7]. Uric acid levels are influenced by age and sex. It has been reported that increased levels of uric acid are associated with established cardiovascular risk factors, such as elevated serum triglyceride and cholesterol concentration, hypertension, obesity, insulin resistance and metabolic syndrome. For that reason, it is one of the factors for inflammatory progression and represents a marker of atherosclerotic disease. The role of uric acid as a risk factor for vascular diseases and acute stroke is controversial; yet, there is little information available about it. Many studies, including the NHANES study, concluded that uric acid is an independent risk factor for development of cardiovascular and cerebrovascular diseases. In contrast, the Framingham Heart Study concluded that an association between hyperuricemia and cardiovascular diseases merely reflects the link between serum uric acid and other risk factors, including hypertension, renal disease, elevated lipoprotein levels and the use of diuretics [4], [3]. In Vietnam, there is no study available about relationship between serum acid uric and ischemic stroke’s prognosis.
Objective:
1)To evaluate serum uric acid concentration in acute ischemic stroke patients.
2) To define correlation between serum acid uric concentration and NIHSS, ischemic size, mRankin
II. RESEARCH DESIGN AND METHODS:
A total of 84 patients aged from 18 years old, admitted to the Cardiovascular Department at Hue Central Hospital, were evaluated in a prospective study from May 2015 to October 2016.
1.Patients
Selection of cases:Cases of acute ischemic stroke admitted to Cardiovascular Department, Hue Central Hospital were included in the study. According to WHO (World Health Organization), stroke was defined as “a syndrome of rapidly developing clinical signs of focal or global neurological disturbance, lasting for more than 24 hours”. Only CT brain-proved cases of acute ischemic stroke were included in the study. Of course, patients have agreed to enroll in this study.
Exclusion criteria:
1) Patients have history about head injuries, transient ischemic attack (TIA); 2) Duration of symptoms extending for more than 7 days; 3) Patients receiving drugs affecting SUA levels (diuretics, losartan, allopurinol, probenecid, atorvastatin, fenofbrate); 4) Active infections, Malignancy, Renal or liver disease.
Selection of controls:
We select 30 healthy controls from the enrolled in the study.
Methods
We used a prospective study from May 2015 to October 2016. Questionnaire was used to record demographic data, including age, sex, and history of diseases like diabetes mellitus, hypertension, and Ischemic Heart Disease, Smoking history. Patients was assessed with neurological impairment by NIHSS, mRankin, Glassgow score and biochemical examinations (Routine blood test, Glucose level, bilan lipid, hs-CRP, serum uric acid) were used. Specifically, serum uric acid was measured in day 1, day 3, day 7 of hospital.
Statistical analysis: Statistical analysis was performed with the help of SPSS 16.0 software. It included the usual descriptive and
univariate analysis. Student t test was used to compare continuous variables and χ2 test was used to compare categorical variables. Unadjusted odds ratio with 95% confidence interval and P values were calculated.
III. RESULTS
Out of 84 patients studied, 48 were males and 36 were females. Male : female ratio was 1.3 : 1. The mean age of cases was 70.04 ± 12.45 and the range was 43 to 95.
1.Serum uric acid concentration in acute ischemic stroke
Mean SUA level in cases in day 1, day 3, day 7 were 344.86 ± 64.84 µmol/l, 323.76 ± 57.47 µmol/l, 308.57 ± 42.50 µmol/l, respectively. whereas it was 304.93 ± 38.29 µmol/l for controls. Mean SUA level was signifcantly higher in cases as compared to controls (p < 0.005) only in day 1 and not significant another day (table 1).
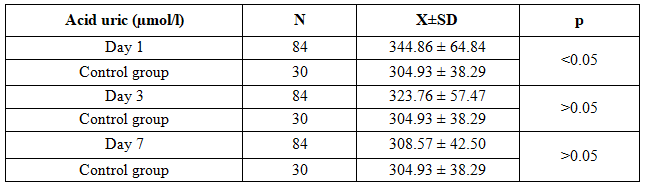 Table 1. Serum uric acid concentration in case – control groups
Table 1. Serum uric acid concentration in case – control groups
In our study, percentage of NIHSS score 0-6, 7-15, ≥16 were 54.8%, 38.1%, 7.1% respectively, and SUA level was higher in patients who had higher NIHSS in day 1, day 3, day 7. However, only day 1 and day 3 recorded a statistically significant difference in SUA levels with p <0.05
(table 2).
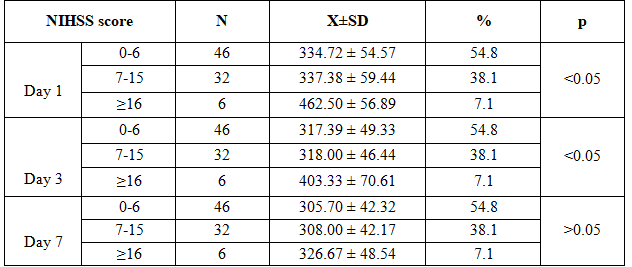
Table 2. Relationship between SUA concentration and NIHSS
Table 3 shows that mRankin score ≤ 2 was 60.71% and mean SUA levels was higher in patients whose mRankin score was > 2. Statistical significant difference was only in day 1.
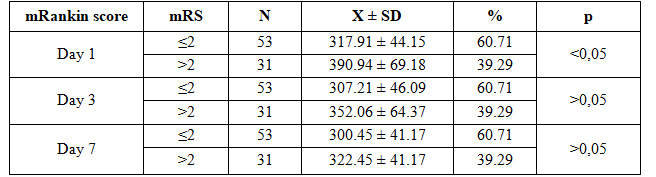
Table 3. Relationship between SUA concentration and mRankin score
Mean SUA concentration was higher in patients who had larger ischemic size. But this difference was not statistically significant as the P value > 0.05 (table 4).
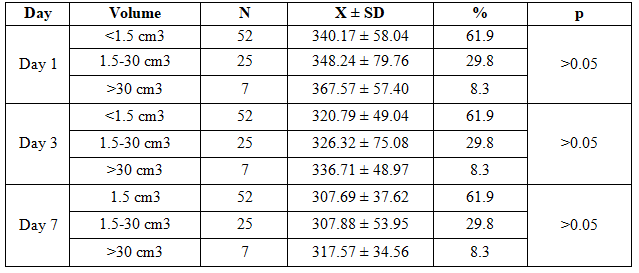
Table 4. Relationship between SUA level and ischemic size in CT scanner
From Table 5, the correlation between SUA and NIHSS score was studied with the help of Spearman rank correlation. It was found that there was a significant positive correlation between SUA and NIH stroke scale score on day 1, as well as day 2 (p < 0.05 for both). But its correlation was weak, recorded as 0.35 and 0.256.

Table 5. The correlation between SUA and NIHSS score
There was a weak significant positive correlation between SUA and mRankin score on day 1 and day 3 (p < 0.01) in Table 6.

Table 6. The correlation between SUA and mRankin score
IV. DISCUSSION
The well-recognized risk factors for stroke, such as age, smoking, diabetes, hypertension, metabolic syndrome, explain only a part of the cases. This study was conducted to study the role of serum uric acid in acute ischemic stroke and its effect on stroke outcome.
The male to female ratio was 1.3:1. The mean age of the cases was 70.04 ± 12.45 years with the range of 43 to 95 years. These findings are consistent with the data published by Pandiyan et al, who observed a male:female ratio of 1.9:1 and mean age of stroke patients as 61.7 ± 13.4 years [1].
Mean SUA level in cases in day 1, day 3, day 7 were 344.86 ± 64.84 µmol/l, 323.76 ± 57.47 µmol/l, 308.57 ± 42.50 µmol/l, respectively, whereas it was 304.93 ± 38.29 µmol/l for controls. Mean SUA level was significantly higher in cases as compared to controls (p < 0.005) only in day 1, and not significantly different on another days. According to Milionis study in acute ischemic stroke of 163 patients, mean SUA was 331.1 ± 101.1 µmol/l and 285.5 ± 83.3µmol/l (p<0,05) [9] in control group.
Rareshwar Koppula study of 550 patients show that hyperuricemia in patient group was 54.9% and 24.7% in the control group. Therefore, our study produces the same results with Milionis and Rareshwar Koppula study.
SUA has been reported that increased levels of uric acid are associated with established cardiovascular risk factors, such as elevated serum triglyceride and cholesterol concentration, hypertension, obesity, insulin resistance and metabolic syndrome. From that reason, it is one of the factors for inflammatory progression, and represents a marker of atherosclerotic disease.
SUA level was higher in patients who had higher NIHSS on day 1, day 3, day 7. But only day 1 and day 3 recorded a statistically significant difference in SUA levels with p <0.05. Rong Li showed there was a statistically significant difference between NIHSS score ≥ 7 and NIHSS < 7, its concentration gradually decreased and return to normal on day 7. It is our theory that this is the probably reason to explain the difference in SUA level on only day 1 and day 3 in our study.
There was a significant positive correlation between SUA and NIH stroke scale score as well as mRankin score on day 1 and day 3 (p < 0.05 for both). But its correlation was weak. SUA and ischemic size demonstrates no correlation in our study. Many study show that increasing SUA levels have poor outcome such as Weir et al: 3731 ischemic patients [11].
V. CONCLUSION
Our findings support the hypothesis that SUA is more a marker of the magnitude of the cerebral infarction, than an independent predictor of stroke outcome.
Mean SUA level in ischemic patients was significantly higher than normal population. It decreased from day 1 to day 3 and day 7: 344,86µmol/l, 323,76 µmol/l, 308,57µmol/l, respectively. There was a significant positive correlation between SUA and NIH stroke scale score on day 1 as well as day 3 (p < 0.05 for both). There was a significant positive correlation between SUA and mRankin score on day 1 and day 3 (p < 0.05).
REFERENCES
- Arjundas Deepak, Uma Pandiyan, G Arjundas, Baux Henry (2007), “Surveillance of stroke: WHO STEP-wise approach: A Chennai stroke unit report”, Annals of Indian Academy of Neurology, 10 (3), pp. 154.
- Barr W. G. (1990), Uric Acid. Editors In: Walker HK, Hall WD, Hurst JW, editors. Source Clinical Methods: The History, Physical, and Laboratory Examinations. Boston: Butterworths.
- Culleton Bruce F., Martin G Larson, William B Kannel, Daniel Levy (1999), “Serum uric acid and risk for cardiovascular disease and death: the Framingham Heart Study”, Annals of internal medicine, 131 (1), pp. 7-13.
- Fang Jing, Michael H Alderman (2000), “Serum uric acid and cardiovascular mortality: the NHANES I epidemiologic follow-up study, 1971-1992”, Jama, 283 (18), pp. 2404-2410.
- Feigin, Valery L, Carlene MM Lawes, et al (2009), “Worldwide stroke incidence and early case fatality reported in 56 population-based studies: a systematic review”, The Lancet Neurology, 8 (4), pp. 355-369.
- Hariklia V, H. V. Dimitroula, Apostolos I Hatzitolios, Haralambos I Karvounis (2008), “The role of uric acid in stroke: the issue remains unresolved”, The neurologist, 14 (4), pp. 238-242.
- Heo Sung Hyuk, Seung-Hoon Lee (2010), “High levels of serum uric acid are associated with silent brain infarction”, Journal of the neurological sciences, 297 (1), pp. 6-10.
- Kim S. Y., JV Guevara, KM Kim (2008), “Hyperuricemia and Risk of stroke: A Systematic Review and Hariklia VD, Apostolos H, Haralambosk. The Role of Uric Acid in Stroke. The lssue Remains Unresolved”, The Neurologist, 14, pp. 238-242.
- Milionis Haralampos J., Evangelos Rizos, John Goudevenos, Konstantinos Seferiadis, Dimitri P Mikhailidis, Moses S Elisaf (2005), “Components of the metabolic syndrome and risk for first-ever acute ischemic nonembolic stroke in elderly subjects”, Stroke, 36 (7), pp. 1372-1376.
- Moreno, Carmen (2010), “Prevalence of stroke and associated risk factors in older adults in Havana City and Matanzas Provinces, Cuba (10/66 population-based study)”, MEDICC review, 12 (3), pp. 20.
- Weir Christopher J., Scott W Muir, Matthew R Walters, Kennedy R Lees (2003), “Serum urate as an independent predictor of poor outcome and future vascular events after acute stroke”, Stroke, 34 (8), pp. 1951-1956.