 Hội Nội Tiết – Đái Tháo Đường Miền Trung Việt Nam Hội Nội Tiết – Đái Tháo Đường Miền Trung Việt Nam
Hội Nội Tiết – Đái Tháo Đường Miền Trung Việt Nam Hội Nội Tiết – Đái Tháo Đường Miền Trung Việt Nam
DEPRESSION. COGNITIVE DISORDER AND QUALITY OF LIFE
IN STROKE PATIENT
Nguyen Dinh Toan
Internal medicine department
Hue University of medicicne and pharmacy
ABSTRACT
Introduction: Stroke is the third most common cause of disability and second most common cause of death worldwide. Depression and cognitive disorder are the important contributions to poor quality of life in stroke.Aim: To evaluate the relationship between the quality of life (QoL) and depression and cognitive disorder in stroke survivors after 3 months.Material and Method:90 patients with stroke were recruited at the Hue Central hospital from July to October 2016. The patients were evaluated using MoCA scale, the Beck Depression Inventory and The WHOQOL-BREF. mRS was used for assessementof the disability level.Results:66.7% of patients had disability (mRS: 2-5).Mean score on the BDI was 19.82 ± 14.03. 58 patients (46.44%) suffered from moderate to severe depression. Demetia rate evaluated by MoCA scale in patient with stroke was 82.2%. Mean score of overall QoL, general health, physical health, psychological health, social relationships, and environmental health was 2.71 ± 0.74, 2.72 ± 0.96, 10.67 ± 2.65, 10.72 ± 2.85, 11.14 ± 1.93 and 11.18 ± 2.89 respectively. The results showed significantly negative correlations between depression, the Activity of Daily Living -ADL scale and quality of life in patients with stroke. Conclusion: Depression and cognitive disorder were principal factors which directly associated with quality of life in stroke patient after 3 months.
Keywords: stroke patient. Beck Depression Inventory. The WHOQOL-BREF. MoCA. MRankin
Main correspondence:Nguyen Dinh Toan
Submission date: 8 Feb 2017
Revised date: 20 Feb 2017
Acceptance date: 15Mar 2017
I. INTRODUCTION
Stroke is the third most common cause of disability and second most common cause of death worldwide. It is one of the most prevalent disorders of old age. and increasing in incidence mainly as a consequence of the growing population of elderly people (Rothwell et al 2004). Improvements in acute stroke care have helped more people to survive the initial event but. while mortality has been reduced. stroke remains a major cause of disability (Hill et al 2009). It often results in major changes in a person’s life: a stroke survivors can suffer loss of health. occupation. social role. and independence (Whyte&Mulsant 2002). Stroke has a huge impact on the patient’s capacity to perform activities of daily living (ADL) (Haghgoo et al 2013). Prevalence of patients who survived stroke and who required care in at least one activity of daily living (ADL) has been estimated in 173/100000 (Bonita et al 1997). ADL involves activities of self-care. such as eating. washing and dressing. and are usually defined as physical self-maintenance tasks.
Depression is an important contribution to poor quality of life. It occurs in about a third of stroke survivors in the first months after stroke (Hackett et al 2006).
Various studies have shown a reduced QoL in patients with stroke compared with healthy individuals (Gunaydin et al 2011).
There are a number of studies who revealed the relation between depression in stroke patients and ADL or QOL (Haghgoo et al 2013; Kwok et al 2006; Herrmann et al 1998; Chong 1995; Carod-Artal et al 2009). Depression has negative effects on the QOL (Kwok et al 2006).
The aim of this study is to evaluate the relationship between the activity of daily living performances and the level of depression. as well as. the quality of life (QOL) in patient with stroke at Hue central hospital
II. MATERIAL AND METHODS
1.Participants
For this study. 90 patients with stroke were recruited at Hue Central Hospital from July to October 2016.
Participants were selected based on the inclusion criteria that consisted of: stroke diagnosis by a neurologist according to the WHO (1983)-criteria and confirmed by clinical history. neurological examination. and imaging via computed tomography or magnetic resonance imaging
2. Instruments
There were four tools for collecting data including:
- A socio-demographic questionnaire who collected data on age. gender. years of education. number of stroke episodes. marital status and history of psychological disorders prior to stroke.
2.The degree of disability was elaluated using The modified Rankin Scale (mRS): 0 – No symptoms.1 – No significant disability. Able to carry out all usual activities. despite some symptoms.2 – Slight disability. Able to look after own affairs without assistance. but unable to carry out all previous activities.3 – Moderate disability. Requires some help. but able to walk unassisted.4 – Moderately severe disability. Unable to attend to own bodily needs without assistance.and unable to walk unassisted.5 – Severe disability. Requires constant nursing care and attention. bedridden. incontinent.6 – Dead.
- The Montreal Cognitive Assessment (MoCA) is a brief screening instrument originally designed to identify MCI in elderly patients attending a memory clinic.4MoCA is a 1-page. 30-point test. administrable in ≈10 minutes. which evaluates different domains: visuospatial abilities. executive functions. short-term memory recall. attention. concentration. working memory. language. and orientation to time and space
- The Beck Depression Inventory (BDI) was used to assess depression among patients (Beck 1961). BDI is a questionnaire who consisted of 21 questions about how the subject has been feeling in the last week. Each question has four possible answer choices based on intensity. including the following scores: zero
(‘’I do not feel sad’’). 1 (‘’I feel sad’’). 2 (‘’I am sad all the time and I can’t snap out of it’’). and 3 (‘’I am so sad or unhappy that I can’t stand it’’). The total score is calculated to determine the depression’s severity. The BDI-II has the standard cut-off points as below: 0–9 no depression. 10-15 minimal depression; 16–19 mild depression; 20–28 moderate depression; and 29–63:severe depression.
- The WHOQOL-BREF is a 26-item instrument consisting of four domains: physical health (7 items). psychological health (6 items). social relationships (3 items). and environmental health (8 items); and two overall QOL and general health items. The physical health domain includes items on mobility. daily activities. functional capacity and energy. pain. and sleep.
The psychologicaldomain measures self-image. negative thoughts. positive attitudes. self-esteem. mentality. learning ability. memory and concentration. religion. and the mental status. The social relationships domain contains questions on personal relationships. social support. and sex life.
The environmental health domain covers issues related to financial resources. safety. health and social services. living physical environment. opportunities to acquire new skills and knowledge. recreation. general environment (noise. air pollution. etc.). and transportation (World Health Organization’s Quality of Life group. US version 1997). All the questionnaire are translated and validated in Vietnamese language.
3. Statistical analysis
Data were analyzed using Statistical Package for Social Sciences (SPSS) version 22
III. RESULTS
1.Demographic characteristics of the study sample
In the study group there were 54.4% males and 45.6% female. Mean age was 65.57 ± 13.38. Almost the patient live in countryside (66.7%). Unemployee was 40%. manual labour was 36.7%.
2. Disability degree following mRS
There were 60 patients had disability with mRS 2-5 (66.7%) and 30 patients were in the range 1-2 (33.33%).
3. Depression rate following the BDI in study group
Based on BDI. there were 58 patients (46.44%) having moderate to severe depression and the remaining 32 (53.56%) were not depressed. Mean score on the BDI was 19.82±14.03
4. MoCA score in study group
Mean MoCA 22.42 ± 2.92. min 17. max 28. There were not differentiation between mean MoCA in ischemic and hemorragic stroke (p>0.05) (table 1).
Table 1. MoCA score in study group
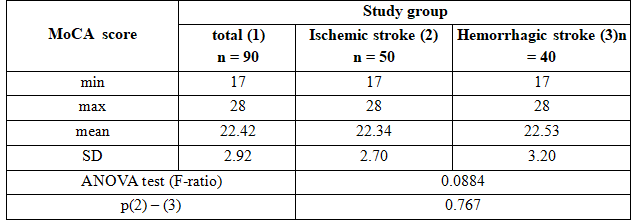 Demetia rate evaluated by MoCA scale in patient with stroke was 82.2%. This rate was higher in the hemorragic stroke group than those in ischemic stroke group but the differentiation was not significant (p>0.05). (picture 1).
Demetia rate evaluated by MoCA scale in patient with stroke was 82.2%. This rate was higher in the hemorragic stroke group than those in ischemic stroke group but the differentiation was not significant (p>0.05). (picture 1).
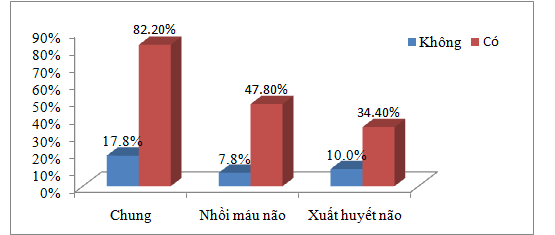
Picture 1. Demetia rate evaluated by MoCA scale in patient with stroke
Table 2. Quality of life in the study group assessed by WHOQOL-BREF
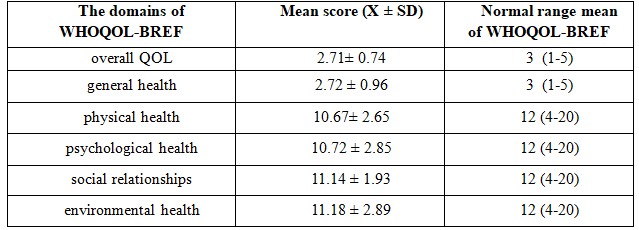
QOL of patient assessed by WHOQOL-BREF in study group were low in all domains compared with the normal range mean
Table 3. The correlation between WHOQOL-BREF with MoCA scale. mRS. BDI
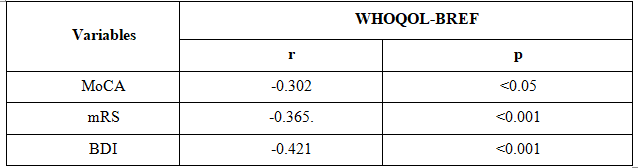 There were a significant negative correlation between WHOQOL-BREF and MoCA scale. mRS. BDI
There were a significant negative correlation between WHOQOL-BREF and MoCA scale. mRS. BDI
Table 4. WHOQOL-BREF scores in stroke patients with and without depression 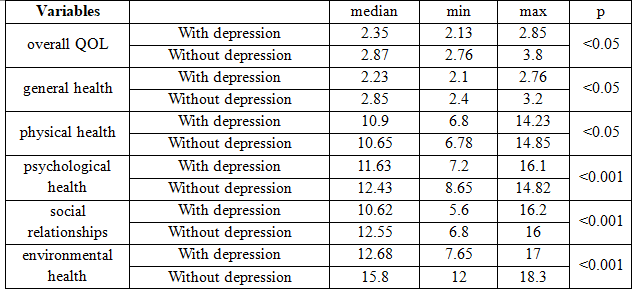
IV. DISCUSSION
Quality of Life (QoL) assessment has been an important part of the evaluation of stroke patients and their treatment for more than 30 years. QoL is difficult todefine and no universal definition of this term exists.
However. there is a general agreement that QoL is a multi-dimensional construct that consists of at least three broad domains: physical. mental and social (Józef A. Opara). In some international studies14-18 using the WHOQOL-BREF instrument. it was observed that the quality of life of an individual is greatly affected after a stroke.
In our study. QOL decreased in all domains compared with the normal range mean (table 2). Mental health. physical and cognitive impairment are related to decreased quality of life. but it is possible to decrease the influence of functional status on the quality of life through social support. education of both patients and members of their families. And suitable support from the community. Patients who can re-integrate into normal life have better outcome of the disease and better quality of life.
In the study by Baune and Aljeesh. it was compared the QoL of hypertensive people with and without CVA. People with stroke had a significantly lower QoL than those hypertensive patients who have not had a CVA. Zalihic et al.15 compared the quality of life of individuals who have suffered a CVA with individuals who have suffered an acute myocardial infarction. The quality of life was significantly worse in patients with stroke compared with those with acute myocardial infarction.
Gupta et al observed in their research with neurological patients. of whom 40% had been affected by a CVA. that the mean scores of the WHOQOL-BREF was lower in the physical domain (38.83) followed by psychological (50.76). social (48.53) and the environment (49.13). Also was concluded that all domains of quality of life are affected and those people affected need to participate in a rehabilitation program. The area most affected in the study by Pan et al.17 was physical. followed by psychological. social relationships and environment.
In the Bölsche et al study the physical domain obtained improval during his intervention. while the social relations domain was most affected.
Demetia rate evaluated by MoCA scale in our study was 82.2%. This rate was higher in the hemorragic stroke group than those in ischemic stroke group but the differentiation was not significant (p>0.05). (picture 1). Pohjasvaara T and al studied on 107 patients with stroke used DSM-IV concluded that dementia rate was 91.6%.
In another study of Cumming TB observed on 294 stroke patients showed that 65% patients having dementia assessed by MoCA scale [3].This rate was 68.2% following the study of Trần Công Thắng [13]
Post stroke depression rate in our study was 46.44% compared with Bao Hung (35.16%). Timothy K 36%. Our result was higher than the others study can explain by mean age was high in the study group. Our result was similar the study of Jönsson AC (41%).
Poststroke depression is a treatable condition; early diagnosis is of paramount importance to prevent progression to a chronic depressive disorder. Depression slows down the process of rehabilitation. exerting a negative influence on all aspects of the process of recovery.
In the table 4. Quality of life evaluated in all items were significantly diffirent between depression group and non-depression group (P<0.05). Quality of life was significantly lower in patients with depression than those without depression. Following Abubakar. Functional status and depression were identified as independent factors affecting Quality of life of stroke survivors.
V. CONCLUSION
It is concluded that stroke has significant impact on the quality of life of survivor post-stroke patients. Depression and cognitive disorder were principal factors which directly associated with quality of life in patient after stroke.
REFERENCE
- S. A. Isezuo2 Health Related Quality of Life of Stroke Survivors:Experience of Stroke Unit. (Int J Biomed Sci 2012; 8 (3): 183-187)
- Trần Công Thắng (2011). “Giá trị của thang điểm mini – cog trong tầm soát sa sút trí tuệ”. Tập san Nghiên cứu Y học Tập 15. (2). tr.83-85.
- Baune BT. Aljeesh Y. The association of psychological stress and health related quality of life among patients with stroke and hypertension in Gaza Strip. Ann Gen. Psychiatry 2006; 5: 6.
- Bölsche F. Hasenbein U. Reissberg H. Schlote A. Wallesch CW. Results of in- vsout patient post-stroke rehabilitation over 6 months. Fortschr Neurol Psychiatr 2003; 71(9): 458-68.
- Cao Phi Phong. Tran Trung Thanh (2013). Evaluation of quality of life after stroke. Y Hoc TP. Ho Chi Minh * Vol. 17 – Supplement of No 1 – 2013: 152 – 157
- Cumming TB et al (2011). “The Montreal Cognitive Assessment: Short cognitive evaluation in a large stroke Trial”. Stroke. (42). pp.2642-2644.
- Gupta A. Deepika S. Taly AB. Srivastava A. Surender V. Thyloth M. Quality of life and psychological problems in patients undergoing neurological rehabilitation. Ann Indian Acad Neurol 2008;11(4): 225-30.
- Pan JH. Song XY. Lee SY. Kwok T. Longitudinal analysis of quality of life for stroke survivors using latent curve models. Stroke 2008; 39(10): 2795-802.
Pohjasvaara T et al (2000). “Comparison of Different Clinical Criteria (DSM-III. ADDTC. ICD-10. NINDS-AIREN. DSM-IV) for the Diagnosis of Vascular Dementia”. Stroke. (31). pp.2952-2957