Hội Nội Tiết – Đái Tháo Đường Miền Trung Việt Nam Hội Nội Tiết – Đái Tháo Đường Miền Trung Việt Nam
Hội Nội Tiết – Đái Tháo Đường Miền Trung Việt Nam Hội Nội Tiết – Đái Tháo Đường Miền Trung Việt Nam
ASSOCIATION BETWEEN SARCOPENIA AND RENAL FUNCTION IN PATIENTS WITH CHRONIC KIDNEY DISEASE
Anh Trung Nguyen 1,2, Thanh Xuan Nguyen1,2, Hong Minh Nguyen3, Huyen Thanh Thi Vu1,2
1National Geriatric Hospital, 2Hanoi Medical University,
3108 Military Central Hospital
DOI: 10.47122/vjde.2021.48.8
ABSTRACT
Objectives: To determine the association between sarcopenia and renal function in patients with chronic kidney disease at the National Geriatric Hospital. Methods: A cross-sectional study included of 180 chronic kidney disease outpatients aged 60 and over who were diagnosed and treatedat National Geriatric Hospital. Sarcopenia was indentified according to National Institutes of Health criteria FNIH. Results: The average age of subjects was 72 ± 8.7 with 65 males and 115 females. The majority of patients in the stage 2 of chronic kidney disease accounted for 50%. The prevalence of sarcopenia was 20.6%. There was a statistically significant association between stage of chronic kidney disease and sarcopenia (p <0.05). Conclusion: The prevalence of sarcopenia in older in-patients with chronic kidney disease at National Geriatric Hospital was rather high, stage of chronic kidney disease was related to sarcopenia.
Keywords: Sarcopenia, chronic kidney disease, elderly
Main correspondence: Anh Trung Nguyen
Submission date: 20th April 2021
Revised date: 26th April 2021
Acceptance date: 26th May 2021
Email: [email protected] Tel: 0903480774
1. INTRODUCTION
Sarcopenia, an age-related decline in muscle mass and function, is one of the most important health problems in elderly with a high rate of adverse outcomes. Based on the results of this meta- analysis, the overall prevalence of sarcopenia was 10%. In Vietnam, the prevalence of sarcopenia according to AWGS criteria was 54.7%, and 40.5% according to FNIH. The prevalence of sarcopenia was significantly higher in men compared with women [1] .
Although sarcopenia was related to aging process, researchers currently recognize the important role of catabolic diseases, such as chronic kidney disease (CKD), in the etiology of sarcopenia [2]. CKD increased in elderly population and some consider it as a new geriatric giant. In fact, metabolic derangements associated with CKD lead to increased protein catabolism, resulting in diminished muscle mass and function, independent of age. Therefore, it can be hypothesized that CKD patients are more prone to develop sarcopenia
Non-dialysis patients with CKD stage 3–5 account for a relatively high proportion, the research and early intervention of these patients may reverse the progression to end-stage renal disease, thus, it has important clinical signicance. To the best of our knowledge, there are few studies on the analysis of sarcopenia in non-dialysis patients with CKD. Sarcopenia is a common disease in elderly patients. To analyze the characteristics of sarcopenia of CKD 3–5 non-dialysis patients is helpful to understand the characteristics of the disease and to control the disease. The aim of this study was to explore the association between sarcopenia and renal function in patients with chronic kidney disease.
2. SUBJECTS AND METHODS
2.1. Participants
Patients aged 60 years or above diagnosed with chronic kidney disease, not on dialysis, visiting the Outpatient Clinics of the National Geriatric Hospital in Hanoi, Vietnam, were recruited from Febuary 2018 to October 2018.
Exclusion criteria were: (1) blind or deaf, (2) severe dementia or delirium, (3) pace-maker implanted and (4) unable to provide consent or refused to participate in the study.
Data were collected from medical records and patient measurement. Information from medical records were extracted using a predefined data collection form, including demographic characteristics (age, gender, Body mass index) and medical history.
Weight (kg): Participants’ weight were measured using an electronic scale, in standing position, minimal clothing and barefoot. Weight was recorded to the nearest 0.1 kg.
Height (m): Participants were measured against a convenient flat wall. Participants were barefoot and height was recorded to the nearest 0.1 cm. Body mass index (BMI) was calculated as weight/height2 (kg/m2) and was categorised into three groups underweight (<18.50), normal (18.50–24.99) and overweight (≥25.00).
Grip strength (kg): Handgrip strength was measured using a dynamometer (Jamar Hydraulic Hand Dynamometer 5030 J1 made in USA). The participants were instructed to sit upright on a chair without armrest, with the elbows flexed at 90°. The measurement was conducted once in the right hand, and once in the left hand. The highest value of the two measurements was used for the analysis.
Muscle mass: Each participant received a whole body dual X-ray absorptiometry scan (DXA Medix DR C12, Mauguio, France) to measure regional lean mass (kg), total body fat (kg) and total body fat percentage (%). Appendicular skeletal muscle (ASM, in kg) was defined as the sum of the lean soft tissue masses of the arms and legs.
2.2. Sarcopenia definition
Sarcopenia was defined as low muscle mass plus low grip strength, using cut-points suggested by the Foundation for the National Institutes of Health (FNIH) [3]
According to FNIH, the recommended cut- points for low grip strength were <26 kg in men and <16 kg in women, and low muscle mass was defined as ASM adjusted for BMI (ASM/BMI)<0.789 in men and <0.512 in women.
Chronic kidney disease was identified and classified according to the criteria of KDIGO (2002), estimated glomerular filtration rate (eGFR) was determined by equation MDRD. Quantification of blood creatinine (micromol unit / l) [4]
Chronic kidney disease was identified and classified according to the criteria of KDIGO (2002), estimated glomerular filtration rate (eGFR) was determined by equation MDRD. Quantification of blood creatinine in units of micromol / l
The International Society of Nephrology (NKF – KDOQI) classifies chronic kidney disease into 5 stages based on GFR (1, 2, 3A, 3B, 4)
2.3. Statistical analysis
Analysis of the data was performed using SPSS for Windows V.20.0 (IBM Corp., Armonk, New York, USA). Continuous variables are presented as mean (±SD), and categorical variables as frequency and percentage. Comparisons between participants with and without sarcopenia were assessed using Χ2 tests for categorical variables and Student’s t-tests for continuous variables. Two-tailed p values<0.05 were considered statistically significant.
3. RESULT
3.1. General characteristics of the participants
A total of 180 elderly patients with chronic kidney disease were included in the study.
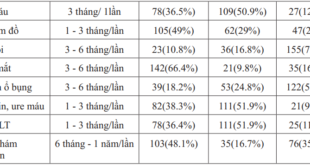
Table 1. General characteristics of the participants (n=180)


In a total of 180 study subjects, the majority of patients are women, accounting for 63.9% (115 patients). Male patients accounted for only 36.3% (65 patients). The female / male ratio is 1.7. The average age of the patients was 72 ± 8.7 years, the majority of patients in the age group from 60 to 69 years old accounted for 41.1%. The majority of patients had a normal body mass index, accounting for 66.7%. The average glomerular filtration rate of the study group was 64.72 ± 16.44 ml / min / 1.73m2. There were 37 patients with sarcopenia, accounting for 20.6%, the proportion of patients without sarcopennia accounted for 79.4% (143 patients).
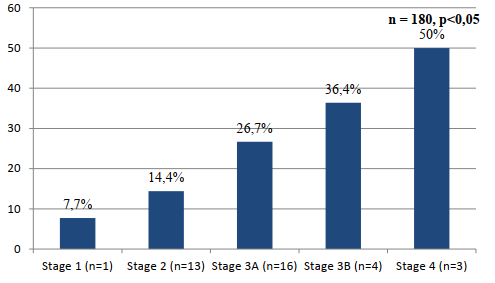
Figure 1. Sarcopenia prevalence by stage of chronic kidney disease
The rate of sarcopenia is proportional to the stage of chronic kidney disease, in which the highest rate is in stage 4, accounting for 50%, stage 3B (36.4%), stage 3A (26.7%), stage 2 (14.4%), the lowest rate of sarcopenia was in stage 1 (7.7%), this difference was statistically significant with p <0.05.
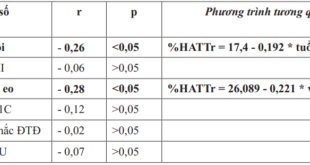
Table 2. Correlation between sarcopenia and glomerular filtration rate (n = 180)

The rate of sarcopenia in the group with the glomerular filtration rate below 45 ml / min is higher than the group with the glomerular filtration rate above 45 ml / min. This difference is statistically significant with p <0.05.
Table 3. Correlation between sarcopenia and albuminuria (n = 113)

In a total of 113 patients tested for albuminuria, the group with albuminuria had a higher rate of sarcopenia than the group without albuminuria. However, this difference is not statistically significant with p> 0.05.
4. DISCUSSION
The study was conducted on 180 outpatients treatment of chronic kidney disease at the National Geriatrics Hospital. The mean age of study patients was 72 ± 8.7 years. The average age in our study is similar to the author’s research in Brazil Vivian et al (2017) with the average age of patients with chronic kidney disease not on dialysis was 73 ± 9 years [5].
In our study, the majority of patients were in stage 2 and 3A of chronic kidney disease, accounting for 50%, 33.3% respectively. In Viviane’s study, patients were mainly stage 3B and stage 4 accounting for 37% and 29% respectively [5]. The results of our study was different from those of the author Viviane because in Viviane’s study, only CKD patients with glomerular filtration rate below 60 ml / min were included in the study. The average glomerular filtration rate of study subjects was 64.72 ± 16.44 ml / min, lower than the Viviane’s study, the average glomerular filtration rate was 35.96 ± 16.01 ml / min.
Among the study patients, 20.6% had sarcopenia according to the FNIH criteria. The rate of sarcopenia between studies is inconsistent, ranging from 5 to 16% at the age of 60 and from 7 to 34% at the age of 70 depending on the study population and sarcopenia diagnostic criteria. Sarcopenia is a rising problem in elderly patients suffering from CKD. Sarcopenic participants with CKD had significant reduction in muscle mass, strength and higher risk of falls which made them more vulnerable to loss of independency and physical inactivity as found by others [6]
In our study, the highest rate of sarcopenia was in stage 4 (50%) followed by stage 3A (33.3%), and the lowest was in stage 1 (7.7%). Thus, most sarcopenia appears in the advanced stages of chronic kidney disease. In addition, our study also showed that the rate of sarcopenia gradually increases with the stage of chronic kidney disease, this difference was statistically significant with p <0.05. Our result was similar to research by Viviane (Brazil, 2017), study by Lagu (USA, 2017) or study by Pereira (Brazil, 2015) [5], [7], [8]. Thus, early intervention in the early stages of chronic kidney disease is needed to limit the progression of the disease, which may prevent the emergence of sarcopenia.
Albuminuria is considered a risk factor for the progression of chronic kidney disease and cardiovascular disease [9]. An association between albuminuria and sarcopenia has been reported in many studies. A National Health and Nutrition Survey of Korea (2011), 2,158 people over 19 years old participating in the study, demonstrated that people with sarcopenia had an increased risk of albuminuria and vice versa [10]. In our study, sarcopenia and albumninuria were not associated. Our results are similar to the results of Viviane et al. (2017), which did not find an association between sarcopenia and albuminuria with a sample size of 100 patients with CKD [2]. This difference is probably due to the fact that our sample size as well as that of Viviane is not large enough to realize the relationship between sarcopenia and albuminuria.
5. CONCLUSION
The prevalence of sarcopenia in older in- patients with chronic kidney disease at National Geriatric Hospital was rather high, stage of chronic kidney disease was related to sarcopenia.
REFERENCES
- Nguyen TN, Nguyen TN, Nguyen AT, et al, (2020). “Prevalence of sarcopenia and its associated factors in patients attending geriatric clinics in Vietnam: a cross- sectional study”, BMJ Open 2020;10 : doi: 10.1136/bmj open-2020-037630
- Souza VA, Oliveira D, Mansur HN, Fernandes NM, Bastos MG, (2015). “Sarcopenia in chronic kidney disease”, J Bras 2015;37(1):98–1. pmid:25923756.
- Chen L-K, Liu L-K, Woo J, et al, (2014). “Sarcopenia in Asia: consensus report of the Asian Working group for sarcopenia”, J Am Med Dir Assoc 2014;15:95–101.
- Chapter 1: Definition and classification of CKD. Kidney Int Suppl (2011). 2013;3(1):19-62. doi:10.1038/kisup.2012.64
- Viviane S , Oliveira D, Barbosa S. R et al (2017). “Sarcopenia in patients with chronic kidney disease not yet on dialysis: Analysis of the prevalence and associated factors”, PloS one, 12 (4), e0176230.
- Foley RN, Wang C, Ishani A, Collins AJ, Murray AM (2007). “Kidney function and sarcopenia in the United States general population: NHANES III”, Am J Nephrol 27(3):279–286.
- Lagu A, Sharma D, Amodu A et al (2017). “Sarcopenia, obesity, and mortality in US adults with and without chronic kidney disease”, Kidney international reports, 2 (2), 201-211.
- Pereira R. A, Cordeiro A. C, Avesani M et al (2015). “Sarcopenia in chronic kidney disease on conservative therapy: prevalence and association with mortality”, Nephrology Dialysis Transplantation, 30 (10), 1718-1725.
- Yuyun F, Khaw T, Luben R et al (2004). “Microalbuminuria independently predicts all-cause and cardiovascular mortality in a British population: The European Prospective Investigation into Cancer in Norfolk (EPIC- Norfolk) population study”, International journal of epidemiology, 33 (1), 189-198.
- Kim T. N, Lee E. J, Hong J. M et al (2016). “Relationship between sarcopenia and albuminuria: the 2011 Korea national health and nutrition examination survey”, Medicine, 95 (3).