 Hội Nội Tiết – Đái Tháo Đường Miền Trung Việt Nam Hội Nội Tiết – Đái Tháo Đường Miền Trung Việt Nam
Hội Nội Tiết – Đái Tháo Đường Miền Trung Việt Nam Hội Nội Tiết – Đái Tháo Đường Miền Trung Việt Nam
LEVELS OF PLASMA HOMOCYSTEINE, FOLATE AND VITAMIN B12 IN HEMODIALYSIS PATIENTS
Hoang Trung Vinh, Diem Thi Van*
*Vietnam Military Medical University
ABSTRACT
Objectives: To evaluate levels of plasma homocysteine (Hcy), folate and vitamin B12 in hemodialysis (HD) patients. Subjects and methods: 112 HD patients in the study group and 56 healthy individuals in the control group had measurement of plasma Hcy, folate and vitamin B12 levels by microparticle chemiluminescent immunoassay in the Department of Biochemistry, 103 Military Hospital. Results: Mean Hcy level in HD patients was 25.43 ± 10.15μmol/l, significantly higher than that of the control group (9.11 ± 2.40 μmol/l, p < 0.001). Mean folate, vitamin B12 levels in HD patients were 12.61 ± 6.74 ng/ml and 635.70 ± 297.52 pg/ml, respectively, not different from those of the control group (12.78 ± 5.43 ng/ml and 600.48 ± 294.49 pg/ml, respectively). 97.3% of HD patients had hyperhomocysteinemia. Majority of the patients had normal folate and vitamin B12 levels. Rates of folate and vitamin B12 deficiencies were 28.6% and 9.8%, respectively. Male patients had a lower level of folate than female (11.50 ± 6.64 vs 15.04 ± 6.38 ng/ml, p < 0.01). Variations of Hcy, folate and vitamin B12 levels in HD patients are not related to age. Conclusions: HD patients had a higher level of plasma Hcy than healthy people while folate and vitamin B12 levels not different from those of normal ones. Rates of hyperhomocysteinemia, folate and vitamin B12 deficiency are 97.3%, 28.6% và 9.8%, respectively.
Key word:Hemodialysis; Homocysteine; Folate; Vitamin B12;
Main correspondence:Hoang Trung Vinh
Submission date: 9 Feb 2017
Revised date: 21 Feb 2017
Acceptance date: 15Mar 2017
1.INTRODUCTION
Homocysteine, a sulfur-containing amino acid normally produced by demethylation of methionine, is an independent risk factor for cardiovascular disease [4]. Hcy is elevated in 85-100% patients with chronic kidney disease (CKD) and negatively correlated with GFR. In cases of advanced CKD and hemodialysis, Hcy level is higher 1.5-2 fold than that of normal people [9], [10].
The mechanisms of hyperhomocysteinemia in CKD are unclear and may include reduced renal metabolism of homocysteine. Relative or absolute deficiencies of folate, vitamin B12 or vitamin B6 have also been proposed because they are essential cofactors for Hcy metabolism [8]. Deficiencies of folate and vitamin B12 in HD patients are caused by many factors such as strict diet, decreased absorption by the intestines, inhibited metabolism and losses through dialysis [5], [10].
Folate and vitamin B12 deficiencies are not only critical factors leading to hyperhomocysteinemia but also important causes contributing to anemia in hemodialysis patients. Therefore, we conducted this study for purpose: To evaluate levels of plasma homocysteine, folate and vitamin B12 in hemodialysis patients.
2.SUBJECTS AND METHODS
2.1.Subjects
168 participants were enrolled in our study and divided into 2 groups: The study group comprised 112 hemodialysis patients at the Department of Nephrology and Dialysis, 103 Military Hospital, from June to October in 2016. And the control group consisted of 56 healthy individuals had age, gender matched with those of the study group.
* Selected criteria for the study group
– We selected hemodialysis patients who had similar methods of treatment (but still had individualizaed) such as having 3 hemodialysis sessions per week, using the same dialyzers with low-flux membranes, using antihypertensive drugs, recombinant human erythropoietin and tardyferol B9.
– ESRD patients with different CKD causes, age and gender.
– Dialysis duration > 1 month.
*Excluded criteria for the study group
– Patients were treated by HDF online method.
– Patients with currently serious complications or malabsorption syndrome.
2.2. Methods
Our study is a cross-sectional description, in comparison with control group.
*Study contents
– For the study group: We collected history of disease, performed clinical examination and laboratory tests. Patients were asked to provisionally stop using folate and vitamin B12-containing drugs at least one day before taking plasma homocysteine, folate and vitamin B12 tests. Blood sample was drawn under fasting condition and before the first dialysis session of the week. Plasma Hcy, folate and vitamin B12 levels were measured by microparticle chemiluminescent immunoassay in the Department of Biochemistry, 103 Military Hospital.
– For the control group: We also asked for history of health and performed clinical examinations of organs. After assessement ofheatlthy individuals, we also measured plasma Hcy, folate and vitamin B12 levels by the same method as in the study group.
*Statistical analysis: Stata 12.0 were used to analyse data. Mean Hcy, folate and vitamin B12 levels of the study group were considered as increases when > X + SD and decreases when < X – SD of the control group.
3. RESULTS
Table 1. Comparing mean age and gender between the two groups
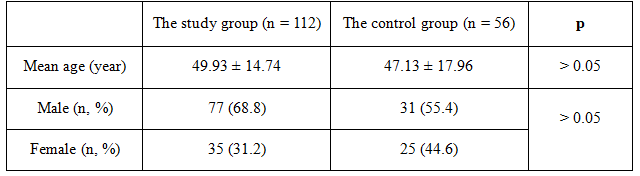 There were no significant differences in mean age as well as gender between the study group and the control group (p > 0.05).
There were no significant differences in mean age as well as gender between the study group and the control group (p > 0.05).
Table2. Comparing mean Hcy, folate,vitamin B12 levels between two groups
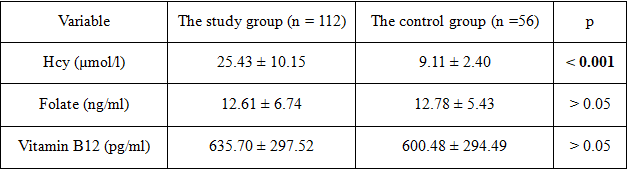 + Mean Hcy level of the study group was significantly higher than that of the control group (p < 0.001).
+ Mean Hcy level of the study group was significantly higher than that of the control group (p < 0.001).
+ There were no statistically significant differences in mean folate and vitamin B12 levels between the two groups (p > 0.05).
Table 3. Distribution of patients by variations of Hcy, folate, vitamin B12 levels (n=112)
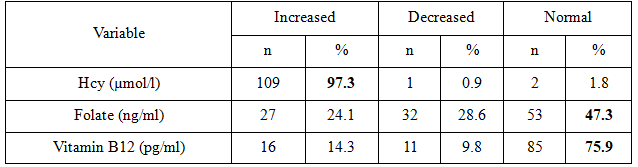 + Most patients had hyperhomocysteinemia, accounting for 97.3%.
+ Most patients had hyperhomocysteinemia, accounting for 97.3%.
+Majority of the patients had normal folate and vitamin B12 levels. Rates of decreased folate and vitamin B12 were not high, accounted for 28.6% and 9.8%, respectively.
Table 4. Variation of plasma Hcy, folate, vitamin B12 levels by age (n = 112)
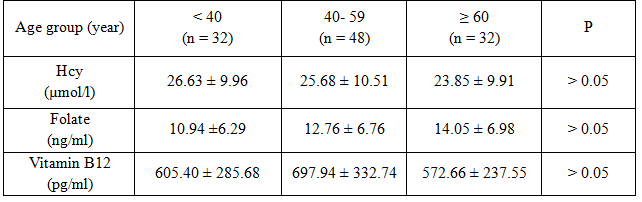 No significant differences were observed in mean Hcy, folate, vitamin B12 levels among age groups (p > 0.05).
No significant differences were observed in mean Hcy, folate, vitamin B12 levels among age groups (p > 0.05).
Table 5. Variation of plasma Hcy, folate, vitamin B12 levels by gender (n = 112)
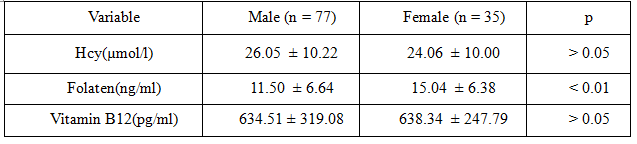 + Mean folate level of female patients was significantly higher than that of male patients (p < 0.01).
+ Mean folate level of female patients was significantly higher than that of male patients (p < 0.01).
+There were no significant differences in mean Hcy and vitamin B12 levels between male and female (p > 0.05).
4. DISCUSSIONS
*Hcy level in hemodialysis patients:There are many causes of hyperhomocysteinemia such as age, gender, malnutrition, drugs, genetic factor, anddiseases leading to hyperhomocysteinemia including CKD. Hyperhomocysteinemia in CKD patients is caused by a decrease in the Hcy elimination by the kidney and inhibition of Hcy metabolism, which is related to folate, vitamin B12 deficiency. Our results showed that mean Hcy level of HD patient was 25.43 ± 10.15 μmol/l, significantly higher than that of the control group (9.11 ± 2.40 μmol/l, p < 0.001) (table 2). Most patients had hyperhomocysteinemia, accounting for 97.3% (table 3). Similar to our findings, Huynh Van Nhuan (2009) reported that mean Hcy level of HD patients was 26.77 ± 12.64 μmol/l, significantly higher than that of the control group (9.56 ±1.92 μmol/l, p < 0.0001) and rate of elevated plasma Hcy level was 89.89% [1]. Moustapha A. et al (1999) also indicated that plasma level of Hcy in HD patients was significantly higher than that of the control group (24.7 – 29.0 vs 10.1-10.9 μmol/l,
p < 0.05) and hyperhomocysteinemia was observed in 90.8% of patients [8].
*Variation of homocysteine level by age, gender: There are many causes that affect plasma level of Hcy, in which age and gender are physiological factors that cause changes in plasma Hcy level. In normal subjects, plasma Hcy level increases with age, males have a higher level of Hcy than female. Lim H. S. et al (2002) studied the concentration of plasma Hcy, folate and vitamin B12 in adults in Korea and reported that mean Hcy levels in men were 11.18 ± 3.88 μmol/l, significantly higher than that in women 9.2 ± 2.65 μmol/l [7].
But in HD patients, our study indicated that there were no significant differences in Hcy level among age groups, between male and female (table 4 and table 5). Similar to our results, Billion S. et al (2002) showed that Hcy level did not differ betweensexes and was not correlated with the age of the patients [3]. De Vecchi A. F. (2000) also indicated that Hcy levels in HD patients did not show statistically significant differences related to gender and age [4]. In HD patients Hcy had no relation to age and sex, which could be explained by Hcy levels in HD patients highly modified by kidney failure and treatment therapy.
*Plasma folate level in hemodialysis patients: Patients receiving regular dialysis may be at risk of developing folate deficiency because foods rich in folate must often be restricted, and the loss of folate across the dialysis membrane is likely to occur because of its low molecular weight and moderate protein-binding ability. Folate metabolism appears to be altered in hyperuremia. Chronic renal failure may impair the intestinal absorption of folate. However, folate losses in hemodialysate were very low compared to total body folate content [6].
Moreover, fortification of cereal grain flour products with folic acid has reduced the prevalence of folate deficency in the general population as well as in HD patients. Many studies in HD patients also reported that folate deficiency is low, in contrast, folate is essentially normal or even increased. Huynh Van Nhuan (2009) found that mean folate level in HD patients was 13.10 ± 7.08 ng/ml, higher than that in the control group (8,13 ± 2,72 ng/ml, p < 0.001) the rates of low and high folate were 4.49% and 11.24%, respectively [1].
Billion S. (2002) reported that average folate level in HD patients was 15.6 ± 8.0 nmol/l, the rate of decreased folate was 10% [3]. Bayes B. (2003) indicated that average folate level was 8.21 ± 4.89 ng/ml, rate of decreased folate accounted for 6.6% [2]. Our results showed that mean folate level of HD patients was 12.61 ± 6.74 ng/ml, not different from that in the control group (12.78 ± 5.43 ng/ml, p > 0.05) (table 2). Majority of patients have normal folate level, accounting for 47.3%. Rates of high and low folate levels were 24.1% and 28.6%, respectively (table 3). Ours findings could be explained by the adequacy of dialysis, by the attention paid in our Unit to folate prescriptions for patients.
*Variation of folate level by age, gender: Lim H. S. et al (2002) studied levels of plasma Hcy, folate and vitamin B12 in Korean adults. The results showed that folic acid level in men was 6.47 ± 3.06ng/ml, significantly lower than that in women (7.96 ± 4.65 ng/ml, p < 0.01) [7].
Research by Shams M. (2009) on folate and vitamin B12 status in healthy Iranian adults showed that serum folate was correlated with age (r = 0.102; p = 0.001) and the average folate level was statistically significantly lower in men than that in women [11]. We founded that in HD patients there were no differences in folate levels among age groups (table 4), but folate level of female was significantly higher than that of male (table 5).
Women have higher folate concentrations than men, which is probably due to women having the habit of eating more vegetables, fruits, mushrooms, legumes than men, which are the foods rich in folate. Moreover men often use alcohol, which can lead to decrease absorption and metabolism of folate.
In healthy people, the folate levels in young people were lower than that of old people, which is probably due to the young people have regeneration of cells and tissues occuring more rapidly than the elderly, so the former demands folate much more. However in HD patients, the concentration of folate did not depend on age anymore, which may be due to folate level in HD patients affected by many factors, especially using folate in treatment.
*Plasma vitamin B12 levelin hemodialysis patients: Vitamin B12 deficiency in CKD and dialysis patients is a controversial issue. According to Chadi Saifan et al, dialysis patients generally have poor nutritional intake, predisposing them to B12 deficiency. In addition, foods that are high in B12 typically contain high concentrations of electrolytes harmful to dialysis patients, limiting them to low B12 foods. Furthermore, B12 is a classic middle size molecule, which is cleared well with modern high flux dialyzers, providing an additional reason for hemodialysis patients to be B12 deficient. However, Fehrman- Ekholm et al failed to show vitamin B12 deficiency in hemodiafiltration patients because he believed that vitamin B12 is a larger molecule than folate (Molecular weight: 1355 Dalton).
In addition, in plasma, it is in protein-bound forms, therefore, losses of vitamin B12 in dialysate are very low[5]. Our findings showed that vitamin B12 level of HD patients were not different from that of the control group (table 2), majority of patients had vitamin B12 levels in normal range (75.9%), rates of patients with increased and decreased plasma vitamin B12 level were 14.3% and 9.8%, respectively (table 3).
Similar to our results, Billion S. (2002) rate of HD patients with reduced vitamin B12 was 6% [3]. De Vecchi A. F. (2000) found that plasma vitamin B12 level of HD patients was 228 ± 478 pmol/l and the rates of decreased and increased vitamin B12 were 10% and 14%, respectively [4]. Bayes B. (2003) reported that rate of decreased vitamin B12 in HD patients was 3.3% [2].
*Variation of vitamin B12 level by age, gender: Absorption of vitamin B12 is pretty complex requiring involvement of many factors such as the gastric PH, gastric intrinsic factor, ileum, transport protein. As age increases leading to poor diet and reduced ability of vitamin B12 absorption which predispose them to a higher risk for vitamin B12 deficiency compared to younger people. Vitamin B12 level is also different between male and female.
Research by Lim H. S. et al (2002) on the concentrations of plasma Hcy, folate and vitamin B12 in adults Korea reported that vitamin B12 level of male (537 ± 222 pg/ml) were significantly lower than that of female (664.1 ± 309.8 pg/ml) [7].
Shams M. (2009) conducted a study on folate and vitamin B12 status in healthy adult Iranians, the results revealed that vitamin B12 was not correlated with age (r = -0.25; p = 0.44) and the mean vitamin B12 level was significantly lower in men than that in women [11].
However, in hemodialysis patients our results showed that there were no differences in mean vitamin B12 levels among age groups, between male and female (table 4 and 5). Similar to our results, Huynh Van Nhuan (2009) found that vitamin B12 levels were not related to ageor sex in hemodialysis patients [1].
5. CONCLUSIONS
Investigating levels of plasma homocysteine, folate and vitamin B12 in 112 hemodialysis patients and 56 healthy individuals, we have the followwing:
– Mean Hcy level in HD patients was significantly higher than that of the control group.
– There were no differences in mean folate and vitamin B12 levels between HD patients and the control group.
-Most patients had hyperhomocysteinemia, accounting for 97.3%.
– Majority of the patients had normal folate and vitamin B12 levels. Rates of folate and vitamin B12 deficiencies were 28.6% and 9.8%, respectively.
– Variations of Hcy, folate and vitamin B12 levels are not related to age.
– Male patients had significantly lower level of folate than female patients.Variations of Hcy and vitamin B12 levels did not differ between male and female.
REFERENCES
- Huynh Van Nhuan (2009), Research on change of blood homocysteine levels and effect of treatment in patients with chronic renal failure on hemodialysis, Medical doctoral thesis, Hue University of Medicine and Pharmacy.
- Bayes B., Pastor M. C., Bonal J., et al. (2003), “Homocysteine, C-reactive protein, lipid peroxidation and mortality in haemodialysis patients”, Nephrol Dial Transplant, 18(1), pp. 106-12.
- Billion S., Tribout B., Cadet E., et al. (2002), “Hyperhomocysteinaemia, folate and vitamin B12 in unsupplemented haemodialysis patients: effect of oral therapy with folic acid and vitamin B12”, Nephrol Dial Transplant, 17(3), pp. 455-61.
- De Vecchi A. F., Bamonti-Catena F., Finazzi S., et al. (2000), “Homocysteine, vitamin B12, and serum and erythrocyte folate in peritoneal dialysis and hemodialysis patients”, Perit Dial Int, 20(2), pp. 169-73.
- Kopple J. D., Massry S. G., Zadeh K. K. (2013), “Vitamin metabolism and requirements in renal disease and renal failure”, Nutritional management of renal disease, pp.351-377.
- Lee E. Y., Kim J. S., Lee H. J., et al. (1999), “Do dialysis patients need extra folate supplementation?”, Adv Perit Dial, 15, pp. 247-50.
- Lim H. S., Heo Y. R. (2002), “Plasma total homocysteine, folate, and vitamin B12 status in Korean adults”, J Nutr Sci Vitaminol (Tokyo), 48(4), pp. 290-7.
- Moustapha A., Gupta A., Robinson K., et al. (1999), “Prevalence and determinants of hyperhomocysteinemia in hemodialysis and peritoneal dialysis”, Kidney Int, 55(4), pp. 1470-5.
- Nand N., Sharma M., Mittal N. (2013), “Prevalence of hyperhomocysteinaemia in chronic kidney disease and effect of supplementation of folic acid and vitamin B12 on cardiovascular mortality”, JIACM, 14(1), pp. 33-6.
- Sarvari G. R., Naseri N., Esmaeeli M., et al. (2014), “Serum Folate and Vitamin B12 Levels in Hemodialysis Patients: Is There any Correlation with Plasma Homocysteine Levels?”, J Ped. Nephrology, 2(4), pp. 140-146.
- Shams M., Homayouni K., Omrani G. R. (2009), “Serum folate and vitamin B12 status in healthy Iranian adults”, East Mediterr Health J, 15(5), pp. 1285-92.